How Your Body and Brain Process Pain

Pain is processed differently, depending on its source.
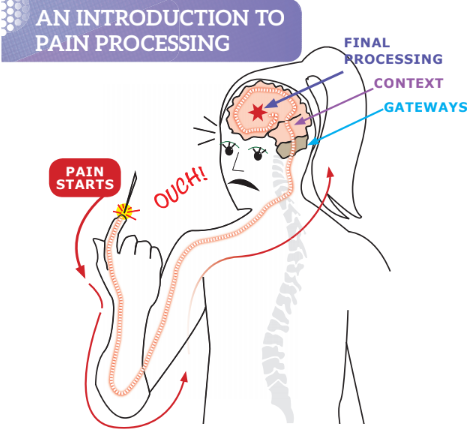
When pain is generated in your body, it is transmitted as a signal to the spinal cord, past several gateways, and then to the brain where it is finally processed. Once the brain decides the signal warrants a response, and what kind of response, it sends a signal back down to the body for a reaction.Here’s a simple diagram:
Copyrighted 2018 When It Hurts Down There
One time, brief pain
When the pain is a one-time or brief event (also called “acute”), the signals follow a path like the one pictured here. For instance, if you burn your left hand with a curling iron, the cell damage in your skin is the instigator of the pain signal. The signal goes to your spinal cord, which sends the signal up to your brain.
If your lower midbrain decides the signal is important, the signal gets passed on to the midbrain. These gateways decide how bad the pain is and relies on the upper brain to confirm: it’s your left hand; the pain is moderately intense; and that it’s a burn and not a cut. The brain then sends a signal to your right hand to move the curling iron away from the skin and to put your left hand under cold water. This all happens in a split second.
When you get the experience of pain over and over again, the brain can’t tell if it’s dangerous, and the nerves in the brain can start overreacting.
For example, the body may think there’s damage, such as inflammation, immune system activation, or an abnormal nerve signal. So the pain-processing nerves in the brain think that they too need more help. They start recruiting their brain neighbors to help process the pain, and make more connections and branches. This “neighboring help” may partly be driven by inflammation and stress that can result in high levels of inflammation chemicals and stress hormones. All this activity from the constant pain can make the brain more sensitive to pain.
With pelvic pain, the brain doesn’t know exactly where the pain signals are coming from. When you have chronic pain in your pelvis, your body may not have to send a signal to the brain to get a reaction. It can just start reacting on its own! And the brain can also get mixed signals from the “neighboring help” and link things like your daily bodily functions, touch, and movement to the pain.
Think of the pain signal in your body acting like a fire alarm.
Chronic, lasting pain
With chronic (constant) pain, weird things happen with the pain signals in the body. When the same nerves in the body have to fire over and over again, they’ll yell for help by releasing nerve-recruiting chemicals.When you get the experience of pain over and over again, the brain can’t tell if it’s dangerous, and the nerves in the brain can start overreacting.
For example, the body may think there’s damage, such as inflammation, immune system activation, or an abnormal nerve signal. So the pain-processing nerves in the brain think that they too need more help. They start recruiting their brain neighbors to help process the pain, and make more connections and branches. This “neighboring help” may partly be driven by inflammation and stress that can result in high levels of inflammation chemicals and stress hormones. All this activity from the constant pain can make the brain more sensitive to pain.
With pelvic pain, the brain doesn’t know exactly where the pain signals are coming from. When you have chronic pain in your pelvis, your body may not have to send a signal to the brain to get a reaction. It can just start reacting on its own! And the brain can also get mixed signals from the “neighboring help” and link things like your daily bodily functions, touch, and movement to the pain.
Think of the pain signal in your body acting like a fire alarm.
 Normally a fire alarm goes off only if there's smoke or a fire. You wouldn’t expect the alarm to sound when you simply light a match or turn on the stove. Normally you wouldn’t expect pain because of average bodily functions, such as having a bowel movement or coughing, or when you have sex. But when your body and brain get overly sensitized to the pain, bodily functions, normal touch, and movement will now cause pain too.
Normally a fire alarm goes off only if there's smoke or a fire. You wouldn’t expect the alarm to sound when you simply light a match or turn on the stove. Normally you wouldn’t expect pain because of average bodily functions, such as having a bowel movement or coughing, or when you have sex. But when your body and brain get overly sensitized to the pain, bodily functions, normal touch, and movement will now cause pain too. As a result, your “alarm” will go off randomly, even when there’s nothing happening!
Seeking help from a pelvic pain specialist is the best approach to help diagnosis and manage pelvic pain. And given the complexity of the pelvic area (See What’s in the Pelvis?), pain is often in more than one site. Your specialist can untangle where your pain is coming from and recommend a course of treatment.
References:
Hampson JP, Reed BD, Clauw DJ, Bhavsar R, Gracely RH, Haefner HK, Harris, RE. Augmented central pain processing in vulvodynia. J Pain. 2013;14(6):579-589.
Janicki T. Chronic pelvic pain as a form of complex regional pain syndrome. Clinical Obstetrics and Gynecology. 2003;46(4):797-803.
Mercier C, Léonard G. Interactions between pain and the motor cortex: Insights from research on phantom limb pain and complex regional pain syndrome. Physiother Can. 2011;63(3):305-314.
Kim W, Kim SK. Neural circuitry remodeling and structural plasticity in the cortex during chronic pain. Korean J Physiol Pharmacol. 2016;20(1):1-8.
Aredo J, Heyrana K, Karp B, Shah J, Stratton P. Relating chronic pelvic pain and endometriosis to signs of sensitization and myofascial pain and dysfunction. Seminars in Reproductive Medicine. 2017;35(1):88-97.
Lee Y, Park K. Irritable bowel syndrome: Emerging paradigm in pathophysiology. World J Gastroenterology. 2014;20(10):2456-2469.
Schrepf A, O’Donnell MA, Luo Y, Bradley CS, Kreder KJ, Lutgendorf S, MAPP Network. Inflammation and inflammatory control in interstitial cystitis/bladder pain syndrome: associations with painful symptoms. Pain. 2014;155(9):1755-1761.
No comments:
Post a Comment